


Safe? And Effective?
How they made me a SKEPTIC

Background. I worked at Queen’s University for >44 years teaching and doing research in Pharmacology with a bit (14 y) of administrative service added in until my retirement in 2017. It’s been a wonderful life both professionally and personally but it was disrupted in January 2020 when all our lives were hit with the declaration of a COVID-19 pandemic. This was met with a government response that has generated a citizen led inquiry and a paucity of academic discourse. (See
https://nationalcitizensinquiry.ca
https://nakatsu.substack.com/p/academic-inquiry-missing-in-action)
As I entered retirement, I had time to read on a lot of different topics, one of which happened to be vitamin D (VitD). Before January 2020, I had learned quite a bit about the sunshine vitamin being essential for much more than bone health as described in many publications by Michael Holick and his research group. Relevant to the issues of Jan 2020, it was well established the VitD was an important factor in our immune systems, in part because of its promotion of the synthesis of cathelicidin and defensin. It was also established that VitD (cholecalciferol) was a pro-hormone and had to metabolized to calcifediol (25-hydroxy-VD) and then further hydroxylated to calcitriol (1,25-dihydroxy-VD), which is the active molecule. A publication that really caught my attention was that of Entrenas Castillo et al (https://pubmed.ncbi.nlm.nih.gov/32871238/ ) who reported that treatment of hospitalized COVID-19 patients with calcifediol was highly beneficial. Thus, of 50 patients treated with calcifediol, only one required ICU admission, while of 26 patients not treated with calcifediol, 13 were admitted to the ICU. Of the former group none died, while two of those not receiving calcifediol died. These observations should have sparked the interest to anyone dealing with COVID-19 patients, i.e. hospitals, doctors, public health officers and provincial politicians.
Or so I thought.
After writing to numerous of the above, I received only one reply- from our local public health officer- whose response can be paraphrased as “I don’t know much about vitamin D”.
While this was disappointing and disconcerting, I kept reading and discovered many published reports on the effectiveness of ivermectin in the early treatment of COVID-19. Most of these arose in developing countries, were modestly funded, and described clinical studies with modest numbers of subjects. The website,
https://c19ivm.org
maintains a complete list of publications on ivermectin in COVID-19.
Of significant relevance was the extremely low incidence of adverse effects attributed to ivermectin. This prompted me to write another round of letters to hospitals, public health officers and provincial politicians. This time the response was even poorer; I didn’t receive any correspondence back from anyone.
It seemed strange that even Merck, the originator of ivermectin, wouldn’t promote the drug even if was only marginally profitable; it had the potential to produce ample good will- much like that produced by giving the Nobel drug away in developing countries for the successful battle against parasitic diseases.
That’s when I remembered the advice, “follow the money”. A quick search of the internet, revealed that Merck had recently received US$356M for developing a new antiviral drug (molnupirarvir) subsequently, they received a contract for US$1.2B. That’s when the lights went on. From that revelation, most of the policies of government, institutions and regulatory bodies started to make sense. I understood that re-purposed drugs and vitamins wouldn’t be big money makers for major corporations, but novel vaccines and anti-virals could be cash cows. I then understood that the “solution” to the pandemic had to be novel (i.e. patent protected) and the darling of the “safe and effective” mantra.
The “vaccine” and me. During my graduate training, 1968-73, I focussed on pharmacology and learned nothing of consequence about vaccinology and immunology. By Jan 2020, I wasn’t much more informed, and I hesitantly took a first Pfizer injection in March 2021. My hesitancy was based on knowing that novel drug approval usually took years, primarily to examine the potential for toxicity in human populations. Between January and June 2021, I had learned enough about immunology and the mRNA shots to tell my family and friends of my concerns. By then I was aware that the “vaccines” were not sterilizing; they couldn’t stop COVID-19 from replicating and spreading. Moreover, reports started to appear saying that the shots were damaging hearts (myocarditis) and women’s reproductive systems. All of this new information made me change my mind; in July 2021, I decided not to take a second injection of mRNA. Needless to say, this decision was met with a mixture of pushback and support. What I’ve learned since then has raised my skepticism as it applies to the mRNA vaccines, and caused me to question our public health authorities, professional colleges, Health Canada, World Health Organization and big Pharma.
Now I tell the story of my journey and some of the evidence encountered on the safety and effectiveness of the mRNA based “vaccines”.
Effectiveness. the USA FDA and Pfizer admitted they do not “stop the spread”.
By August 2021, Dr. Rochelle Wolensky (US FDA) and Janine Small (Pfizer spokesperson to European Parliament) admitted (on TV) that the mRNA vaccines would not stop the spread of COVID-19. Small said that they were working “at the speed of science” implying that there wasn’t time to determine their effect on viral transmissibility. Critically, this meant that the mRNA might only protect the vaccinee but would not prevent the spread to others. I.e. you couldn’t protect Grandma and Grandpa by taking the shot. This made sense because the antibodies raised by the mRNA shots could be found in the general circulation, whereas the virus gained entry via the upper airways mucosa, which was largely inaccessible to the circulating antibodies. Competent vaccinologists predicted this lack of effect against COVID-19 spread.
Why didn’t Big Pharma? Or maybe they did, but calculated that profits could still be made by convincing the World Health Organization (WHO), the regulatory agencies and mainstream medicine that the messiah (aka vaccine) was coming.
Effectiveness- more deaths after vaccines in clinical trial.
Phase 3 clinical trial had more deaths in the vaccinated group than in the placebo group; this shouldn’t happen with an effective vaccine.
This Pfizer-sponsored clinical trial was described as “placebo-controlled, observer-blinded, multinational, pivotal efficacy trial, … 44,165 participants 16 years of age or older … to receive two 30-μg doses, at 21 days apart, of BNT162b2 or placebo.” (Thomas et al, 2021. https://pubmed.ncbi.nlm.nih.gov/34525277/) It was claimed that vaccination resulted in 91.3% protection against contracting COVID-19. But this was the relative risk reduction; the absolute risk reduction was 3.6%. There were 15 deaths in the BNT162b2 group and 14 in the placebo group during the blinded 6-month phase; after this, some members of the original placebo group received BNT162b2. For all subjects receiving vaccination 20 died, and for the unvaccinated there were 14 deaths. This is not statistically significant because you can’t detect the effect of vaccination among just 34 deaths. But vaccination had not resulted in fewer deaths.
Effectiveness- deaths went up rather than down after the vaccine rollout.
But what about the larger population of vaccinated who were not part of the clinical trial; by this I mean those who were given the mRNA injections as part of the vaccine rollout. What does all-cause mortality tell us? Here is a graph of excess deaths for 2020 into 2023, from Our World in Data; it shows that after Canada had vaccinated over 80% of the population, deaths were still about 10% higher than expected.

Effectiveness- more boosters resulted in more COVID-19. A study from the Cleveland Clinic revealed that the cumulative incidence of COVID-19 was higher in people with more doses. 4 doses> 3 doses> 2 doses> 1 dose> 0 doses. Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine - PubMed (nih.gov)

So the shots didn’t “stop the spread” and they didn’t save lives. Were they safe? Let’s look at the evidence.
Safety- the toxicity trials were stopped.
As we have seen above the Pfizer blinded clinical trial was ended after 6 months, meaning that the toxicity monitoring that was supposed to occur in an unbiased manner couldn’t be done. This means that there cannot be a complete blinded documentation of the vaccine adverse effects. This resulted the adverse events occurring after the general distribution of vaccines were recorded on a voluntary basis whereby medical staff and patients may have reported problems after vaccination. This is most problematic because the Canadian procedure for reporting adverse effecst actively discouraged submission of reports. I know doctors who tried to report adverse effects and had the majority of their reports rejected by the public health agencies. This suppression of toxicity data biased reports in favour of vaccine safety. Even in the US FDA’s Vaccine Adverse Events Reporting System (VAERS) only about 1% of adverse events were recorded.
Safety- Reports of heart and brain toxicity
In the spring of 2020, cases of myocarditis and pericarditis began to be reported, especially among teenaged boys and young men. Blood clots were reported after vaccination.
While myocarditis was initially considered to be rare, as a Danish study reported an absolute rate 1.4 per 100 000 vaccinated individuals within 28 days of vaccination (95% confidence interval 1.0 to 1.8). This was based on clinically recognized myocarditis. More recent studies (in Thailand and Switzerland) that used troponin to determine (subclinical) myocarditis revealed that the rate is about one in 35 recipients of mRNA injections. I interpret this as death of some cardiac cells; we won’t know the extent of harm until these subjects reach old.
Safety. The shot didn’t stay in the arm.
Evidence from Japan revealed that the “vaccine” did not stay in the muscle where it was injected. Experiments in rats showed that it was distributed throughout the body. Disturbingly the reproductive organs, ovaries and testicles, accumulated the shot.
Safety. Personal confirmation of risk to other organs.
A family friend told me that her adult daughter and female friends developed changes to their menstrual cycles shortly after taking the vaccine. This is anecdotal evidence but I can’t ignore it.
Just the tip of the Ice Berg. The above examples were just the early warnings that I picked up; much more was detected in subsequent months by many others using other tools. Here is more evidence that we should be concerned about the lack of safety.
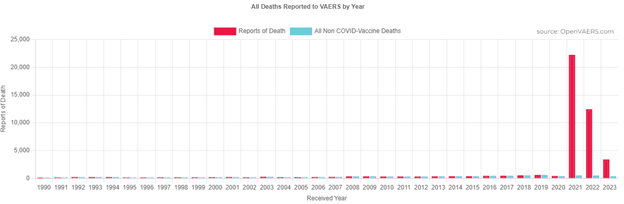
Deaths from VAERS. After the COVID-19 vaccines were rolled out in the USA, total deaths due to vaccinations exceeded all vaccine related deaths in the previous 30 years as shown in the graph below.
Toxicity data from the United Nations VigiAccess system.
COVID-19 vaccines were reported as contributing 5,260,861 adverse events the three years from 2020 Dec to 2023 Dec 16; this compares to 239,536 for combined diphtheria, pertussis, tetanus vaccine in over 40 years from 1981 to 2023 Dec 16.
New Zealand data previously kept secret by their government and released by whistleblower, Barry Young, indicates that the death rate among COVID-19 vaccinees was 1 per 1000.

Questionable Quality Control of Vaccines.
Many reports have been made raising questions about the quality of the mRNA preparations that have been injected in the arms of people everywhere.
For starters, the mRNA that was used in the Pfizer clinical trials was made by one method, while the mRNA for public vaccination was made by a substantially different method. In method one, the production process employed the cleaner RT-PCR technique to create the DNA templates for mRNA transcription. For method two, the large-scale manufacturing process involved growing E.coli to produce the mRNA. The latter is associated with multiple questions of quality assurance including batch to batch variability, low mRNA purity and contamination with DNA. See https://onlinelibrary.wiley.com/doi/10.1111/eci.13998
https://osf.io/preprints/osf/mjc97
Book on Toxicity of mRNA Vaccines. See Michael Palmer et https://doctors4covidethics.org/mrna-vaccine-toxicity/ The authors have released their 235 page book entitled “mRNA Vaccine Toxicity” and made it freely available to the public.

Summary.
Now I am a Skeptic. I entered the COVID-19 pandemic knowing little about the disease and the SARS-CoV2 virus. Almost 4 years later, I know more but cannot call myself an expert because there is so much to learn. It is important for all citizens to learn more about everything that affects us, our family and our fellow citizens.
I used to accept news on the CBC as being mostly accurate- Now I am a skeptic.
I used to accept “information” from Health Canada as being accurate- Now I am a skeptic.
I used to accept universities as being places where all concepts could be challenged- Now I am a skeptic.
I used to accept the World Health Organization as being concerned about our health- Now I am a skeptic.
In my next entry, I plan to explore the failure of Canadian institutions.